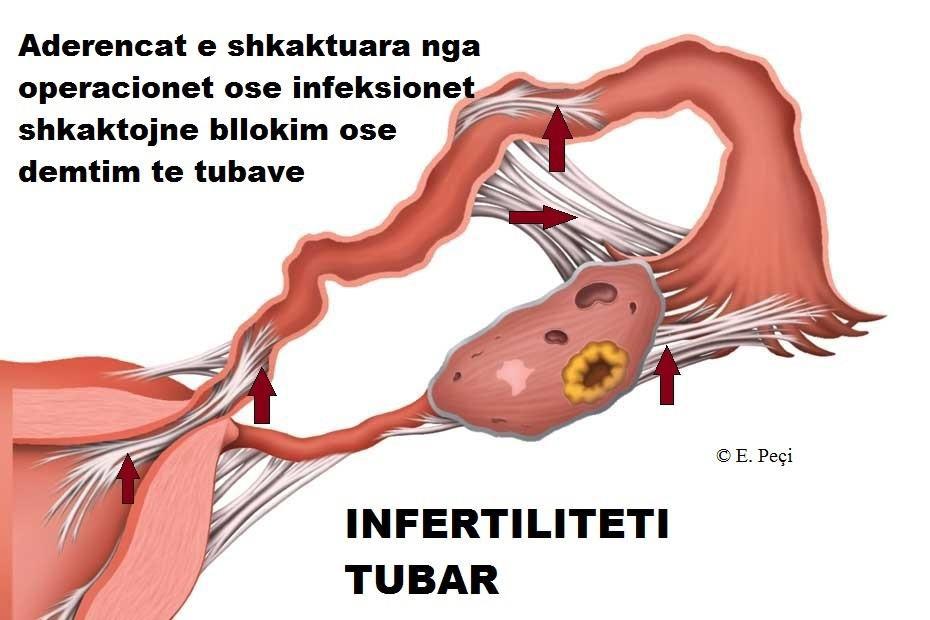
TUBAL INFERTILITY (When the tubes do not function properly)
In a portion of infertile couples, infertility is tubal in consequence. Meaning, the Fallopian tubes are blocked or do not function properly.
Damage is usually caused by the formation of scars or adhesions that can occur as a consequence of pelvic endometriosis, various surgeries (cesarean delivery, acute appendicitis, peritonitis, etc). These adhesions make the meeting of the egg (ovum) and sperm (which normally meet in the tubes) impossible.
Different infections, like chlamydia, can damage cilia (tiny structures in the form of eyelashes or flagella inside the tube) which help in the transport of the egg. If these cilia do not function normally, then the tube, despite possibly being open, does not facilitate the meeting of the egg with the sperm or even if the egg meets the sperm and embryo formation occurs, the latter cannot pass through the tube and enter the uterus to implant.
This last variant leads to the implantation of the embryo outside the uterus; thus the so-called ectopic pregnancy (extrauterine). Other infections that can cause tubal damage include gonorrhea and all those causing pelvic inflammatory disease.
Another form of tubal infertility (although rare) is that which comes as a consequence of tubal ligation (cases where women intentionally close their tubes at a certain point in life (to not have children anymore) and later, as time passes, change their mind because they want to have children again.
How is tubal infertility diagnosed?
Tubal infertility is diagnosed through the following procedures:
Hysterosalpingography – HSG. HSG is a technique that uses X-rays and the injection of a contrast inside the uterus and tubes to see if the latter are open or not.
Laparoscopy. Laparoscopy is an invasive technique aimed at diagnosis and / or surgical treatment inside the abdomen without the need for its classic surgical opening. This is achieved through the insertion into the abdomen of a probe at the level of the navel which contains a high-quality camera. Through 2-3 other accessory holes in the lower part of the abdomen, other instruments can be inserted depending on the problem the patient presents. For checking the tubes during laparoscopy, their external appearance is evaluated (whether they are in normal shape, whether they are free or caught in adhesions, etc) and whether their trajectory is open by injecting a contrast called methylene blue from the vagina. If the tubes are open, then the contrast injected from the vagina will come out inside the abdomen.
How can tubal infertility be treated?
Minor damages to the tubes. Laparoscopy can treat minor problems of the tubes; for example cutting the adhesions that deform the tubes or position them in abnormal places.
Major damages to the tubes. If the tubes are damaged and completely blocked, then through open surgery they can be repaired by removing the blocked part and joining the healthy parts. Theoretically this may seem easy, but practically this is a technique that brings very little success in restoring the normal function of the tubes. The site of rejoining, healing like any wound in the body, might leave scars which can cause narrowing or even blocking of the tube in the same place.
This is the reason why in cases with severe damages to the tubes, their surgical treatment is abandoned due to low success, giving way to in vitro fertilization. Tubal damage is also the standard classic indication for in vitro fertilization (a technique in which the tubes are not involved).
In cases where the woman has intentionally closed her tubes, what is the possibility that they can be reopened through surgery?
Theoretically, this is possible through open surgery (laparotomy). Tubal ligation is treated the same as severe tubal damages (see above). Returning the tubes to their original function is very unlikely.