Knee Prosthesis. (Part One)
Knee prosthesis is a surgical procedure that improves the quality of life and eliminates pain in many patients with severe knee osteoarthritis. Pain and the decrease in quality of life are the two main factors for undergoing this procedure (according to the Arthritis Foundation in the USA).
Generally, patients undergo this procedure after all non-operative treatments (such as daily activity modification, anti-inflammatories, intra-articular injections) have failed to ease the pain. Knee prosthesis has been widely used for more than three decades, generally with excellent results (in the majority of studies, a success rate of over 90% is reported after 10 years).
There are two types of knee prostheses
- Total Knee Prosthesis (Three-Compartmental Prostheses)
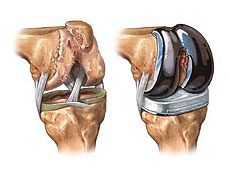
- Unicompartmental Knee Prostheses (mini knee)

Both types have very good results (in terms of longevity and clinically).
Generally, Knee Prostheses have a 7–10 cm anterior incision, hospital stay of 3–5 days, and a healing period (during which the patient walks with crutches or a cane) that ranges from 1–6 months. Most patients report substantial or complete relief from osteoarthritis symptoms after undergoing knee prosthesis. Elimination of pain is considered a liberating factor for many patients who undergo this procedure.
Unicompartmental Prostheses, like Total Prostheses, offer excellent clinical results, but only a small portion of patients with arthritic problems (about 10%) are suitable candidates for this procedure.
Etiology
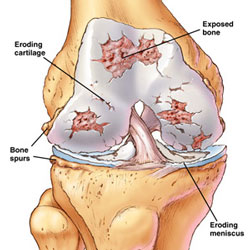
Osteoarthritic injuries of the knee are the main reasons for Total Knee Prosthesis. This is a disease of the synovial joints, characterized by degenerative and reparative processes, and observed in 40% of radiological examinations in patients ≥ 40 years old. However, only 50% of these patients are symptomatic. Osteoarthritis can be primary or secondary.
Mechanical injuries (such as previous meniscus or Cruciate Ligaments injuries), pyogenic infections, ligament instability, and intra-articular fractures are the most common causes of secondary osteoarthritis. Other causes of cartilage injuries include rheumatoid arthritis, hemophilia, pigmented villonodular synovitis, idiopathic avascular necrosis and steroids, and rarely bone dysplasia.
Risk factor studies for severe osteoarthritis of the hip and knees have shown that siblings of people who have undergone joint prostheses have a 3-5 times higher probability than people of the same age as them, to need the same surgical intervention. This means that genes contribute about 30% to the total risk for severe Osteoarthritis.
Laboratory-based studies have shown that chromosome 11 is associated with severe hip osteoarthritis and chromosome 2 with severe knee osteoarthritis. The exact genes involved are not yet known.
Pathophysiology
The exact causes of degenerative processes in primary osteoarthritis are unknown. They may represent a defect in the cellular repair process (chondrocytes). Osteoarthritic cartilage has been seen to contain increased amounts of water; alterations in the type of proteoglycan; abnormalities in type II collagen; and low levels of cathepsin, metalloproteinase, interleukin-1, and other components of the enzymatic process cascade.
Changes in the synovia include: hyperplasia of the synoviocytes, an increase in the leukocyte population in the membrane and fluid, occasionally giant cells, revascularization with an increase in vascular permeability, and alterations in matrix formation and cellular cytokines.
Disease Presentation
The clinical history in a patient with knee arthritis is dominated by pain. This usually occurs during weight-bearing but in the final stages the pain can be constant and not relieved by rest. Night pain is a symptom that requires attention. The pain can be localized in one compartment or spread throughout the knee. Other symptoms include joint stiffness, swelling, and a sensation of giving way.



The patient is asked about the maximum walking distance, the use of stairs (mainly climbing) and what was the first appearance of patella-femoral injuries, the need for assistance or support while walking, the ability to dress/undress themselves and to take care of themselves, and the ability to perform activities requiring knee flexion.
Some patients may feel a significant interference of this disease in their social life, sexual function, sleep, and may feel tired or depressed because of their condition.
The integrity of the ligaments is checked because their deficiency may require the use of special prostheses with intrinsic stabilization.
It is necessary to continuously search for and exclude other origins for knee and leg pain. These include discopathies and other spinal diseases, pain radiated from the ipsilateral hip joint, peripheral vascular diseases, meniscopathies, and knee bursitis.
Thank you for the information you provide us. But I have a question. I had a total knee replacement in November 2012 and in December 2014, I slipped on snow and all of my body weight fell on the operated knee (the healthy knee did not touch the ground) the same situation repeated itself also before a month when I slipped again. I am interested to know if these impacts have any negative effect on the lifespan of the prosthesis? Please give me an answer, thank you Ani Terova
Sent by ani terova, më 22 May 2015 në 08:45