Idiopathic Scoliosis in Children and Adolescents (Part One)
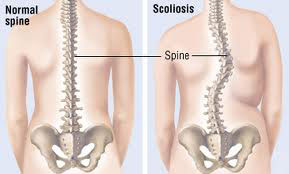
Scoliosis is called the deformation that comes as a result of a lateral curvature of a segment of the spinal column against its longitudinal axis, making it appear in the shape of "S" or "C" which normally should be straight and have the shape of "I".
Scoliosis can cause the vertebrae (rings) to rotate, causing one shoulder or hip (buttock) to be higher than the other.
The term "idiopathic" means that the cause of this disease is unknown.
Therefore, Scoliosis represents the lateral and rotational distortion of the spinal column. We are dealing with a 3-dimensional damage. Sometimes the rotation also determines a deformation of the thoracic cage and the organs contained in it (heart, lungs, and diaphragm).
Classification of Scoliosis:
Scoliosis can occur at any age.
Classification according to age:
- Idiopathic Adolescent Scoliosis occurs after the age of 10. It is the most common type.
- Juvenile Scoliosis occurs in children between the ages of 3 and 10. This is not common.
- Infantile (female) Scoliosis occurs in children younger than 3 years old. This may result from congenital abnormalities of the vertebrae, various syndromes, neurological disorders, or for unknown reasons (idiopathic).
Classification according to cause:
- 80% of them are idiopathic (without a known cause).
- Congenital Scoliosis, originating from defects in organogenesis during the embryonic period.
- Neuromuscular Scoliosis (from poliomyelitis, osteodystrophy, etc).
Epidemiology:
The frequency of scoliosis:
Scoliosis is about 7 times more common in females than in males, and most often appears in ages from 3 to 10 years old.
5% of the world population is affected, of which 81% the causes are unknown, 15% congenital and about 10% neuromuscular.
A Scoliosis curve measured at least 10° occurs in 1.5% to 3.0% of the population.
A curve exceeding 20° occurs in 0.3% to 0.5% of the population.
A curve exceeding 30° occurs in 0.2% to 0.3% of the population.
Small spinal curves occur with similar frequency in boys and girls, but girls are more likely to have a large progressive scoliotic curve that will require treatment.
Symptoms:
Scoliosis usually does not cause any pain, neurological dysfunction, or breathing problems. Concern over the cosmetic appearance of the back is often the main concern of the patient and parents. So, it is a slow and progressive disease, generally asymptomatic. Often it's the parents or the pediatrician who first notice that something has changed in the child's posture. In rare cases, there may be concerns in the spinal column or muscle fatigue after physical exertion. Generally, the child is calm, sleeps well, and continues to perform his/her daily activities normally.
Diagnosis:
Doctor's examination:
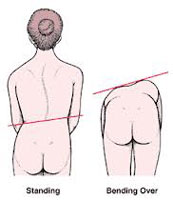

The doctor will ask your child to bend forward, which will show any deformation. This is called the "Adam's Forward Bend Test". The doctor will also check for any discrepancies in limb length, abnormal neurological findings, or other possible causes.
Investigation and tests:
Many schools regularly conduct scoliosis screening for students. These screenings are usually done during middle school and 9th grade years. Your child may receive a recommendation for scoliosis from a doctor based on the school screening results. A differential diagnosis should be made between anatomical scoliosis with rotation, and so-called "functional scoliosis", which is a pathology that is much simpler to treat, as it does not have bone defects at its base.
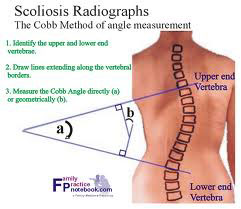
Scoliosis is confirmed by an x-ray of the spine. Your doctor will measure the degree of the curve, as shown in the x-ray.