Quadriceps Tendon Rupture (Part Four)
Non-surgical Treatment
Small and partial tears generally respond well to non-surgical treatment.

Immobilization. Your doctor may recommend that you use a knee immobilizer or brace. This will keep your knee straight to help it heal. You will most likely need to use crutches to help you avoid putting full weight on the leg. The knee immobilizer or brace is worn for 3 to 6 weeks.
Physical therapy. Once the pain and swelling have stabilized, physical therapy can be started. Specific exercises can maintain strength and range of motion.
Exercises will be gradually added to your program. Lifting the leg straight up to strengthen the quadriceps is the most important exercise in physical therapy. As time progresses, your doctor or therapist will increase the range of motion at the brace. This will allow you to move more freely with a greater range of motion. You will be given more strengthening exercises as you heal.

Your doctor will discuss with you when it is safe to return to sports activities.
Depending on your age, activity, and previous level of function, your doctor may recommend surgery for large or partial tears or partial tears associated with tendon degeneration.
Surgical Treatment
Most people with a completely torn tendon require urgent surgery to repair the torn tendon. Surgery is also an option for patients with a partially torn tendon who also have weakening and degeneration of the tendon.
Surgical repair reattaches the torn tendon to the top of the kneecap. Patients who undergo surgery do well if the repair is performed early after the injury, that is, in an early phase. Early repair can prevent the tendon from becoming fibrotic or shortened.
Hospital stay. Most patients will stay in the hospital for at least one night after this operation.
The operation can be performed under regional (spinal) anesthesia or under general anesthesia (breathing tube). It cannot be done under local anesthesia.
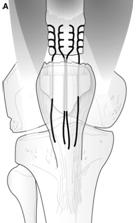
Procedure. To reattach or reconnect the tendon, hooks (sutures) are applied to the tendon and then inserted through several holes drilled in the kneecap. The hooks are tightened or tied firmly at the end of the kneecap, with the proper tension.
New technique. A recent development in the repair of the quadriceps tendon is the use of suture anchors. Surgeons use suture anchors to stitch the tendon to the top of the kneecap. Using these suture anchors means that holes in the kneecap are not needed. This is a new technique, so research data do not yet have conclusions about its effectiveness. Most orthopedists are applying the classic technique for repairing the quadriceps tendon, namely direct repair -- stitching with holes by drilling the kneecap.
Complications. The most common complications of quadriceps tendon repair include weakness and loss of motion. In addition, the position of the kneecap may be different after the operation.
As with any surgery, other possible complications include wound infection, slow healing, blood clots, or anesthesia complications.
Rehabilitation. After the operation, you will need pain management, including ice and medications. About 2 weeks after the operation, the skin stitches will be removed.
A knee immobilizer or a long circular cast will be necessary. You may bear weight on the leg with the help of crutches. Over time, your doctor will increase the degree of the brace. This will allow you to move more freely with a greater range of motion. Strengthening exercises will be added to your rehabilitation plan.
The exact timeframe for physical therapy and the type of exercises prescribed will be individualized for you. Your rehabilitation plan will be based on the type of tendon tear you have, surgical repair, health condition, and your needs.
Complete healing takes at least 4 months. Most patients are healed around 6 months. Many patients have reported that it took them 12 months to achieve all their goals.
Outlook
Most people are able to return to their previous professions. Slightly more than half of the people experience thigh weakening and mild pain at the tendon site. Patients who undergo surgery are better off if the repair is done early after the injury.
If you are a competitive athlete, the surgeon will test the strength of your leg before you return to sports activities. The surgeon will compare the strength of your thigh/leg by using several functional tests on the knee. The goal is for the strength to be at least 85-90% of the uninjured side. In addition to leg strength, the surgeon will evaluate your leg balance and whether you have had any swelling.
Your return to competitive sports status will be carefully discussed with you by your surgeon.