The selection of the best embryo for transfer in an In-vitro Fertilization program.
During in-vitro fertilization (IVF), there are three important factors in achieving pregnancy: the rate of embryo division, morphological quality, and the number of embryos transferred. After egg retrieval, the maturity of the egg and its morphology are good initial predictors for the possibility of having embryos after intracytoplasmic sperm injection (ICSI).
From birth, all eggs are arrested at an early stage (prophase I) of the first meiotic division known as the primary oocyte (primordial follicle). With the onset of puberty, throughout each menstrual cycle, the day before ovulation, the pituitary gonadotropins stimulate the completion of the first meiosis. The secondary oocyte is in the second meiosis (appearance of the first polar body) but is arrested in metaphase and will NOT proceed further if fertilization does not occur.
During fertilization, the second meiosis is completed by forming the second polar body.
At the moment of egg retrieval during IVF, we can capture eggs in three developmental stages: Germinal Vesicle (GV), Meiosis I (M1), and Meiosis II (M2). (Fig.1)

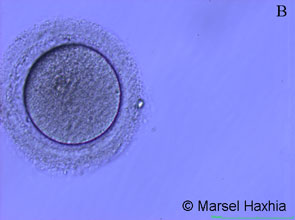

Fig.1 Photos taken from the Embryology laboratory at American Hospital, Tirana. A- egg in GV phase; B- egg in M1 phase; C- egg in M2 phase.
These are microscopic views of oocytes which we classify as mature phase M2 and immature phase GV and M1. From the eggs in the M2 phase, fertilization is expected after ICSI, but in our practice at the American Hospital, we perform ICSI also for M1 eggs to increase the fertilization rate, although it is proven that the latter is much lower than in M2 eggs.
There is a general tendency to pay little attention to egg morphology in the process of embryo selection for transfer. (Ebner et al., 2006a). It is thought and suggested that the quality of the oocyte will have an impact on the implantation rate and clinical pregnancy (Serhal et al., 1997; Loutradis et al., 1999). However, this is still a debatable topic today. To facilitate the study, oocyte dysmorphisms are divided into extra-cytoplasmic and cytoplasmic anomalies (Mikkelsen and Lindenberg, 2001; Ebner et al., 2006a).
In extra-cytoplasmic anomalies, changes in shape, color, size of the perivitelline space, anomalies of the polar body, or the zona pellucida are included. In cytoplasmic dysmorphisms after ovarian stimulation for IVF, two types of anomalies are reported to have a negative influence on the future fate of the egg: firstly, Ebner and his colleagues (in 2005) found that there was a significant decrease in fertilization in eggs that have a vacuole with a diameter greater than 14 µm and secondly, Otsuki and his colleagues (in 2004) showed that the presence of aggregates of smooth endoplasmic reticulum in the cytoplasm is associated with a decrease in the likelihood of having a successful pregnancy.
In conclusion, we can say that the maturity of the egg at the moment of retrieval after ovarian stimulation and cytoplasmic dysmorphisms such as the presence of vacuoles with a diameter > 14 µm and the presence of aggregates of the smooth endoplasmic reticulum in the cytoplasm are very important predictors for the further course of the egg and the selection of the embryo for transfer.
After the ICSI procedure, we can observe signs of fertilization 18-22 hours after ICSI. At this stage, the presence of pronuclei facing each other and/or early division is a sign that indicates the embryo has better chances of implanting. We can observe the development of day 2, 48 hours after ICSI, 2-4 cells, and 72 hours after ICSI is the day three phase with 6-8 cells. The day five embryo phase is only reached by embryos of better quality. (Fig.2) The fact that the embryo reaches the blastocyst phase is an indicator of a higher chance for pregnancy.




Fig.2. Photos taken from the Embryology laboratory at American Hospital, Tirana. A- embryo 18-20h after ICSI, pronuclei phase; B- embryo 48h after ICSI, 2-4 cell phase; C- embryo 36h after ICSI, in the 6-8 cell phase; D- embryo on day five, blastocyst phase.
Very important characteristics in evaluating the embryo quality before transfer are: the division rate - division should be according to the phase in which the embryo is, the size of the blastomeres - their sizes should be equal among them, the level of fragmentation - it has been proven that a fragmentation level < 10% does not affect the pregnancy rate, and the thickness of the zona pellucida – which should not be more than 10 µm.
All of the above are practiced in our daily work at the American Hospital, achieving significant successes. In over 600 IVF treatment cycles in 2 and a half years, we have managed to have a fertilization rate of 67%, a pregnancy rate of 51%, and a birth rate of 73%.
All these results have also come as a consequence of following the best international protocols for selecting the best embryo or embryos for transfer. Determining the day of transfer and the number of embryos to be transferred is also a decision that is tailored to each patient's specific clinical case.
a very good and dedicated doctor with soul
Sent by ari, më 25 November 2014 në 08:38