Clubfoot - Twisted foot or Pes Equinovarus (Part Two)
TREATMENT
The aim of the treatment of Pes Equinovarus (PEV) is to reduce or completely eliminate the components of the foot deformity so that the patient has a fully functional, painless, plantigrade foot with good mobility and without calluses, and does not need to wear special shoes.
Conservative (non-surgical) treatment
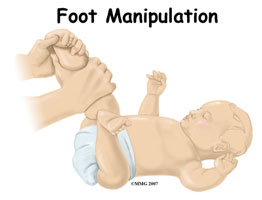
Treatment should start immediately to have the best chance for a successful outcome without the need for surgery. Over the last 10 - 15 years, success has increasingly been achieved in correcting clubfoot without the need for surgery. A particular method of stretching and casting known as the Ponseti method. With this method, the doctor changes every week for several weeks, always doing stretching and casting towards the correct position. The Achilles tendon is then cut followed by a plaster cast for three weeks.
Once the foot is corrected, the infant must wear a brace at night for two years to maintain the correct position. This has been extremely effective, but requires active participation from the parents in daily care by applying the brace. Without parental participation, the twisted foot will almost certainly recur. This is because the muscles around the foot can pull it back into an abnormal position.
The aim of this, and any treatment program, is to make your newborn's twisted foot (or feet) functional, painless, and stable until they are ready to walk. (Note: Whenever your child is put in a cast, look for changes in skin color or temperature that may indicate circulation problems)
 |
 |
Summary:
So, corrective exercises and application of immobilizing plaster at weekly intervals according to the Ponseti method.
The corrective exercise program includes correcting all elements of the deformity, the adduction of the forefoot, varus and equinus of the hindfoot.
The corrected position is maintained with plaster. This action is always carried out until the foot can be dorsiflexed and everted above the neutral position.
In cases of resistant equinus, percutaneous tenotomy is indicated. Radiological examination of the talocalcaneal angle serves for the accurate verification of the deformity correction.
Subsequent treatment then continues with the Dennis-Brown splint connected to sandals and aims to maintain the corrected position.
 |
 |
Surgical treatment
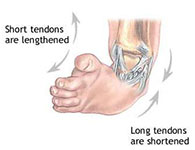
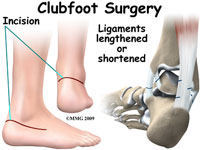
In some cases, stretching, casting, braces are not enough to correct your child's twisted foot, hence the presence of residual deformity and the inability to maintain a satisfactory corrected position. Surgery may be necessary to correct the tendons, ligaments, and joints in the foot/ankle.
The operation is usually done at the age of 9 -12 months of the child, the surgery corrects all the deformities of your child's twisted foot at the same time. After the operation, the foot is placed in a cast until it heals. It is still possible for the muscles in your child's feet to try to return to the twisted foot position, hence it is recommended to wear special shoes or braces for a year or more after the operation. Unfortunately, the operation results in a more rigid foot compared to non-surgical treatment.
Without any treatment, your child's twisted foot will result in severe functional disability. With treatment, your child should have an almost normal foot. The child can run and play without pain and wearing normal shoes. However, a corrected twisted foot will not be perfect. You should expect the child to have a size 1 -1/2 smaller and less mobile than a normal foot. The muscles of your child's twisted foot will also be smaller in size.
 |
 |
 |
According to Salter, about 60% of cases with PEV treated early non-operatively with the above-mentioned methods respond well to treatment within the first three months.
The remaining 40% are resistant to these methods and, as a consequence, in such circumstances, the continuation of conservative treatment leads to incomplete correction of the deformity and recurrent deformity. In these cases of resistant PEV, it is better to perform surgical intervention on the soft tissues at this time rather than to wait for operative intervention because later the operative intervention is larger and its result less satisfactory.
Cases of neglected and recurrent PEV always require surgical treatment, the extent of which depends on the degree of presence of different components of residual deformity.
In general, soft tissue operations (such as capsulotomy, tendon lengthening, tendon transposition) are effective in the first five years of life but become less effective in older children due to the increasingly abnormal shape of the bones. For this reason, in older children, bone operations (such as subtalar and mediotarsal joint arthrodesis) are usually necessary to correct any residual deformity, but it is better to postpone until around ten years of age.
Recently, it has been emphasized that early minor operations for PEV at three months of age have significantly reduced the number of recurrent cases and are an important factor in improving the overall treatment outcome for this significant congenital anomaly such as the subcutaneous tenotomy according to Ponseti.
Is there a cure for my slightly curved legs, meaning below the knee my shin is not straight? In other words, can I make my shin straight, and if so, how?
Sent by Anisa, më 12 April 2018 në 12:14
For sure, there is treatment... you can come so we can consult closely
Replay from Dr. Ledian Fezollari, më 12 April 2018 në 13:17